Medical history.

The medical history or anamnesis (abbr. Hx) of a patient is information gained by a physician by asking specific questions, either of the patient or of other people who know the person and can give suitable information (in this case, it is sometimes called heteroanamnesis), with the aim of obtaining information useful in formulating a diagnosis and providing medical care to the patient. The medically relevant complaints reported by the patient or others familiar with the patient are referred to as symptoms, in contrast with clinical signs, which are ascertained by direct examination on the part of medical personnel. Most health encounters will result in some form of history being taken. Medical histories vary in their depth and focus. For example, an ambulanceparamedic would typically limit his history to important details, such as name, history of presenting complaint, allergies, etc. In contrast, a psychiatric history is frequently lengthy and in depth, as many details about the patient's life are relevant to formulating a management plan for a psychiatric illness.
The information obtained in this way, together with clinical examination, enables the physician to form a diagnosis and treatment plan. If a diagnosis cannot be made, a provisional diagnosis may be formulated, and other possibilities (the differential diagnoses) may be added, listed in order of likelihood by convention. The treatment plan may then include further investigations to clarify the diagnosis.
Process
A practitioner typically asks questions to obtain the following information about the patient:
- Identification and demographics: name, age, height, weight.
- The "chief complaint (CC)" - the major health problem or concern, and its time course (e.g. chest pain for past 4 hours).
- History of the present illness (HPI) - details about the complaints, enumerated in the CC. (Also often called 'History of presenting complaint' or HPC.)
- Past Medical History (PMH) (including major illnesses, any previous surgery/operations (sometimes distinguished as "Past Surgical History" or PSH), any current ongoing illness, e.g. diabetes).
- Review of systems (ROS) Systematic questioning about different organ systems
- Family diseases - especially those relevant to the patient's chief complaint.
- Childhood diseases - this is very important in pediatrics.
- Social history (medicine) - including living arrangements, occupation, marital status, number of children, drug use (including tobacco, alcohol, other recreational drug use), recent foreign travel, and exposure to environmental pathogens through recreational activities or pets.
- Regular and acute medications (including those prescribed by doctors, and others obtained over-the-counter or alternative medicine)
- Allergies - to medications, food, latex, and other environmental factors
- Sexual history, obstetric/gynecological history, and so on, as appropriate.
- Conclusion & closure
History-taking may be comprehensive history taking (a fixed and extensive set of questions are asked, as practiced only by health care students such as medical students, physician assistant students, or nurse practitioner students) or iterative hypothesis testing (questions are limited and adapted to rule in or out likely diagnoses based on information already obtained, as practiced by busy clinicians). Computerized history-taking could be an integral part of clinical decision support systems.
Review of systems.
Whatever system a specific condition may seem restricted to, it may be reasonable to review all the other systems in a comprehensive history. The review of systems should include all the main systems in the body that may provide an opportunity to mention symptoms or concerns that the patient may have failed to mention in the history. Start with the review of systems as following: -Cardiovascular system(chest pain, dysponea, ankle swelling, palpitations) are the most important symptoms and you can ask for a brief description for each of the positive symptoms. -Respiratory system (cough, haemoptysis, wheezing, pain localized to the chest that maight increase with inspiration or expiration). -Gastrointestinal system (change in weight, flatulence and heart burn, dysphagia, abdominal pain, vomiting, bowel habit). -Genitourinary system (frequency in urination, pain with micturition, urine color, any urethral discharge, altered bladder control like urgency in urination or incontinance, menstruation and sexual activity). -Nervous system (Headache, loss of consciousness, diziness and vertigo, speech and related functions like reading and writing skills and memory). -Cranial nerves symptoms (Vision, diplopia, facial numbness, deafness, oropharyngial dysphagia, limb motor or sensory symptoms and loss of coordination). -Endocrine system (weight loss, polydipsia, polyuria, increased appetite and irritability). -musculoskeletal system (any bone or joint pain accompanied by joint swelling or tenderness, aggavating and reliefing factors for the pain and any positive family history for joint disease). -Skin (any skin rash,recent change in cosmetics and the use of sunscreen creams when exposed to sun).

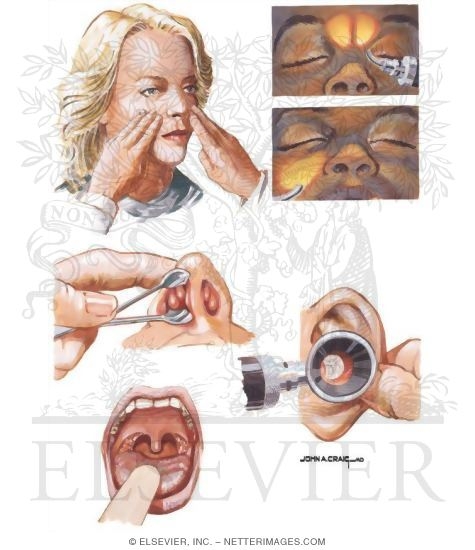
Physical examination.
A physical examination, medical examination, or clinical examination (more popularly known as a check-up or medical) is the process by which a doctor investigates the body of a patient for signs of disease. It generally follows the taking of the medical history — an account of the symptoms as experienced by the patient. Together with the medical history, the physical examination aids in determining the correct diagnosis and devising the treatment plan. This data then becomes part of the medical record.
Medical uses.
A physical examination may be provided under health insurance cover, required of new insurance customers, or stipulated as a condition of employment. This is a part of the insurance medicine. In the United States, physicals are also marketed to patients as a one-stop health review, avoiding the inconvenience of attending multiple appointments with different healthcare providers. Comprehensive physical exams of this type are also known as executive physicals, and typically include laboratory tests, chest x-rays, pulmonary function testing, audiograms, full body CAT scanning, EKGs, heart stress tests, vascular age tests, urinalysis, and mammograms or prostate exams depending on gender. The executive physical format was developed from the 1970s by the Mayo Clinic and is now offered by other health providers, including Johns Hopkins University, EliteHealth and Mount Sinai in New York City.
While elective physical exams have become more elaborate, in routine use physical exams have become less complete. This has led to editorials in medical journals about the importance of an adequate physical examination. In addition to the possibility of identifying signs of illness, it has been described as a ritual that plays a significant role in the doctor-patient relationship. Physicians at Stanford University medical school have introduced a set of 25 key physical examination skills that were felt to be useful.
No hay comentarios:
Publicar un comentario